Drugs for the Prevention and Treatment of COVID-19 and its Complications: An update
What we learned in the past two years

Statement by the Lincei Committee on Covid-19
Executive Summary
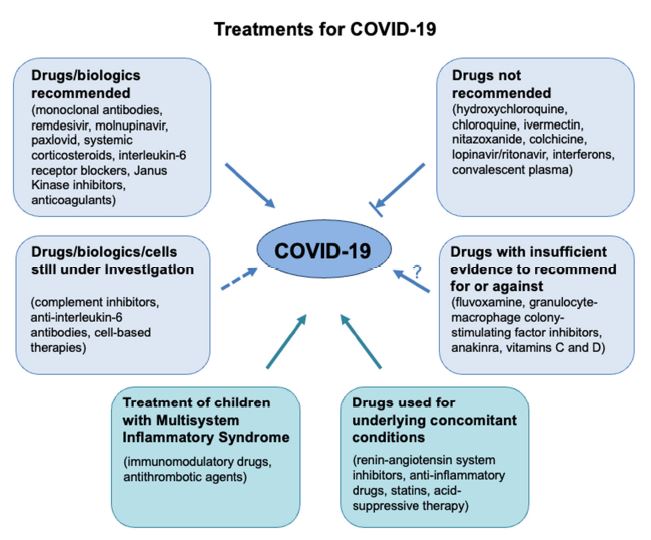
The COVID-19 Committee of the Lincei Academy has updated the reviewed evidence for the efficacy and safety of repurposed and new drugs for the prevention and treatment of COVID-19 and its complications, as well as the safety of some concomitant medications.
A number of pharmacological strategies could theoretically prevent the entry of SARS-CoV-2 into target cells and are currently being evaluated for efficacy and safety. These include neutralizing antibodies against the SARS-CoV-2 spike protein, a soluble recombinant form of the SARS-CoV receptor angiotensin-converting enzyme (ACE)2, and drugs inhibiting the activity or expression of the transmembrane protease serine 2 (TMPRSS2) required for the spike protein proteolytic cleavage. A problem with the use of neutralizing antibodies has been the rapid emergence and spread of mutations of the spike protein, which are not recognized by available antibodies. Regarding the use of convalescent plasma for treatment of COVID-19 in hospitalized patients, it is not recommended in those without impaired humoral immunity.
Remdesivir was identified early as a promising therapeutic candidate for COVID-19 because of its ability to inhibit SARS-CoV-2 in vitro. Based on the results of a double-blind, placebo-controlled RCT of intravenous remdesivir in 1,063 adults hospitalized with COVID-19 with evidence of lower respiratory tract involvement, which demonstrated that remdesivir was superior to placebo in shortening the time to recovery in this setting, in 2020 the US Food and Drug Administration (FDA) has made remdesivir available under an emergency-use authorization (EUA) for the treatment of adults and children with severe COVID-19 disease (May 1st), followed by approval for use in adults and pediatric patients requiring hospitalization (October 22nd). On January 21 2022, based on new evidence, the FDA authorized remdesivir also for outpatient treatment of people at high risk of COVID-19 disease progression, and expanded the pediatric EUA to include treatment of nonhospitalized pediatric patients at high risk. In addition to remdesivir, in the last months two new antiviral drugs, molnupiravir (Lagevrio), and ritonavir-boosted nirmatrelvir (Paxlovid), received an EUA in different countries. Both drugs are available for oral use in non-hospitalized patients, with mild to moderate COVID-19 at high risk of developing severe disease. However, several factors may limit their use: molnupiravir might be able to cause mutations in human DNA, leading the health authorities in some countries to advise against its use during pregnancy, while other countries have chosen not to authorize it. Regarding paxlovid, its possible interaction with a wide range of commonly used drugs may limit its use
Early in the course of the SARS-CoV-2 pandemics, it was claimed that nonsteroidal antiinflammatory drugs (NSAIDs), like ibuprofen, could aggravate the infection by masking its symptoms. However, after review of the evidence, the WHO and EMA advisories have been withdrawn. Therefore, until we have robust evidence, patients in chronic pain should continue to take their NSAIDs rather than turn to opiates. Given that the elderly comprises an at-risk group for severe COVID-19, an association between NSAIDs and the disease may merely reflect reverse causality. Low-dose aspirin appears minimally effective in patients hospitalized with COVID-19. Its utility in patients with milder disease remains to be reported.
The benefit of corticosteroids in the treatment of COVID-19 has been established in large clinical trials in hospitalized critically ill patients, showing a significant reduction of mortality as compared to those allocated to usual care. The usefulness of dexamethasone in patients with severe pulmonary complications of COVID-19 infection has been confirmed by a recent WHO metaanalysis. Based on this evidence, the use of dexamethasone in hospitalized patients requiring respiratory support is widely recommended.
Several observational studies and randomized controlled trials have been performed with immunomodulatory drugs, particularly those targeting IL-6 and its downstream signaling, such as the Janus kinase (JAK) and signal transducer and activator of transcription (STAT) pathway. Based on available evidence, the FDA issued an emergency authorization for the use of tocilizumab in combination with corticosteroids in hospitalized adult and pediatric patients (two years of age or older) with COVID-19 who require supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation. Clinical trials involving several JAK inhibitors for the treatment of COVID-19 are ongoing, and their results will hopefully provide valuable information on the usefulness of these agents.
The complement system is one of the host immune system’s first line defense against invading pathogens. Collectively, early clinical findings and emerging clinical trial evidence suggests the potential therapeutic benefits of some complement inhibitors in severe COVID-19. The results of ongoing phase II/III clinical trials will elucidate the benefit to risk profile of complement inhibitors, clarify the optimal target(s) in the complement cascade, and characterize which patients may benefit the most.
Dysregulation of the coagulation cascade and fibrinolytic system is emerging as an important pathophysiologic component of COVID-19. Largely based on observational studies, the International Society on Thrombosis and Haemostasis (ISTH) suggested measuring D-dimer, prothrombin time and platelet count in all COVID-19 patients. ISTH also recommends that all COVID-19 patients admitted to hospital be treated with prophylactic doses of low-molecular-weight heparin, unless contraindicated. Moreover, recent available evidence from RCTs supports the concept that therapeutic dose anticoagulation with low-molecular-weight heparin or unfractionated heparin is associated with improved outcomes in hospitalized patients with COVID-19 who are not critically ill or in the ICU setting, particularly in those with elevated D-dimer levels. There is not yet consensus on the role of extended thromboprophylaxis beyond the hospital stay. Additional RCTs of several antithrombotic agents are currently ongoing.
Earlier, the FDA had also issued an EUA allowing the temporary use of hydroxychloroquine (HCQ) and chloroquine (CQ) during the COVID-19 pandemic for treatment of the virus in hospitalized patients when clinical trials are not available, or participation is not feasible. This decision was largely based on mechanistic considerations and political pressure. Subsequent observational studies and a limited number of RCTs have not substantiated the clinical efficacy of these antimalarial drugs, while confirming their dose-dependent cardiac toxicity. At present, the US National Institutes of Health (NIH) COVID-19 Treatment Guidelines recommend against the use of CQ or HCQ for the treatment of COVID-19. In addition, the recent NIH guidelines have also indicated a list of drugs that are not recommended for the COVID-19 treatment because of proven lack of efficacy, including the anti-parasitic ivermectin, colchicine, and interferons.
Several other drugs are still in clinical trials, and, considering the preliminary results, there is insufficient evidence to recommend for or against their use in COVID-19 patients. Among these, anakinra, an interleukin-1 receptor antagonist. While the SAVE-MORE trial in hospitalized patient with moderate or severe COVID-19 pneumonia, reported a lower risk of clinical progression of the illness in patients given anakinra than in those receiving placebo, the REMAP-CAP, an open-label, adaptive platform, randomized controlled trial, showed no efficacy of the drug in reducing the combined endpoint of in-hospital mortality and day of organ support.
In view of the current understanding of the pathophysiologic mechanisms of COVID-19 and the unique biological characteristics of mesenchymal stromal cells (MSC), the development of this celltherapy has been seen as a promising approach for patients with SARS-CoV-2 infection, especially for those with severe illness. However, data supporting cell-based therapy with MSC in COVID-19 patients are limited to small open-label studies and few randomized control trials. Nonetheless, so far, no MSC products have been approved by the FDA for the treatment of COVID-19.
Individuals with underlying chronic conditions, such as cardiovascular disease (CVD), pulmonary disease, diabetes, and malignancy are at high risk for severe illness with COVID-19. These patients are usually prescribed medications to treat these disorders. Although ACE inhibitors and angiotensin-receptor blockers (ARBs) may enhance ACE2 gene expression, an effect that would increase the availability of receptor molecules for SARS-CoV-2 entry, there is no evidence that these commonly used drugs might be harmful in patients with COVID-19. Therefore, persons with COVID-19 who are prescribed ACE inhibitors or ARBs for cardiovascular disease (or other indications) should continue these medications. Similar approach will be adopted for the use of statins. Thus, according to the NIH COVID-19 Treatment Guidelines Panel, patients with COVID-19 who are treated with concomitant medications for an underlying medical condition should not discontinue these medications during the acute management of COVID-19, unless discontinuation is otherwise warranted by their clinical condition. In addition, there is recommendation against using medications off-label to treat COVID- 19 if they have not been shown to be safe and effective for this indication in a randomized clinical trial.
Finally, during the first peak of COVID-19 pandemic in Europe, multisystem inflammatory syndrome in children (MIS-C) was first described in reports of children presenting with a severe multisystem hyperinflammatory illness temporally associated with preceding SARS-CoV-2 infection or exposure. The pathogenesis of MIS-C is still being elucidated. However, given the reported clinical similarity between MIS-C to Kawasaki’s disease, the approach to treatment of MIS-C has been similar to that of Kawasaki’s disease, the most commonly used therapy being intravenous immunoglobulin (IVIG) and glucocorticoids. There is also agreement that MIS-C children should also be given low-dose aspirin.
Responsibility for the information and views expressed in this document lies solely with the Covid-19 Committee.